Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 5
Open Access
Volume 5
Antigoni Delantoni, DDS, MSc, Phd, MD1*; Apostolos Sarafopoulos, MD2; Nikolleta Pyrrou3; Vasileios Rafailidis4; Dimitrios Andreadis5
*Corresponding Author: Antigoni Delantoni
Faculty of Dentistry, Aristotle University of Thessaloniki, Greece.
Email: andelant@dent.auth.gr
Article Info
Received: Dec 07, 2024
Accepted: Jan 09, 2025
Published: Jan 16, 2025
Archived: www.jclinmedsurgery.com
Copyright: © Delantoni A (2024).
Abstract...
This paper aims to present a case of IgG4 sialadenitis.
Case presentation: The case presented is a histologically verified IgG 4 sialadenitis where the patient presented with unilateral gland swelling. High frequency ultrasound (6-15 MHz) was used for examination along with color doppler technique.
Kuttner tumor is a multi-organ, immune-mediated fibroinflammatory disease that may affect almost any organ. Unlike Sjogren syndrome, kuttner tumor almost exclusively affects the submandibular gland. It is a benign condition that presents as a palpable mass that can mimic neoplasia.
Conclusions: Ultrasound examination of the salivary glands contributes significantly to the diagnosis autoimmune sialadenitis whether IgG4 or other. Though it is an operator-dependent method and in early stages others methods may be needed for the diagnosis.
Keywords: Kuttner’s tumor; Ultrasonography; Diagnosis; IgG4 sialadenitis.
Citation: Delantoni A, Sarafopoulos A, Pyrrou N, Rafailidis V, Andreadis D. Kuttner’s Tumor Ultrasonographic characteristics. A Review of the Literature Based on a Case. J Clin Med Surgery. 2025; 5(1): 1181.
Introduction
Enlargement of the submandibular gland is a condition that alarms the patient and alerts the medical practitioner for further investigation. There are many possible conditions where the submandibular gland may present a swelling, one of which is a relatively newly described condition of IgG4 autoimmune sialadenitis which presents clinically in the submandibular gland as a pathological condition known as Kuttner’s tumor. The condition is also referred to as chronic sclerosing sialadenitis. It is an autoimmune reaction, non-neoplastic and almost solely presenting in the submandibular gland.
Case presentation
Clinical findings: A 56-year-old male with Ig4 disease and a known history of chronic pancreatitis presented with a painless, palpable very firm non-tender hard mass in the left submandibular gland.
Diagnostic intervention: During the ultrasound examination, a hypoechoic nodule was revealed on the anterior surface of the salivary gland, with a compact texture and the presence of central vascularity. This is a typical case of a “Kuttner tumor”. Longitudinal sections show multiple nodules converging on the periphery of the left gland and not just the palpable nodule. The right submandibular gland shows in the largest part a pathological texture with reduced echogenicity of homogeneous distribution (Figure 1).
Surgical intervention: The lesion was operated on and removed. Histology showed preservation of architecture, septa with fibrotic tissue, atrophy of sections of the glandular acini, and an inflammatory infiltrate of lymphocytes and plasma cells. This set the diagnosis of Kuttner’s tumor.
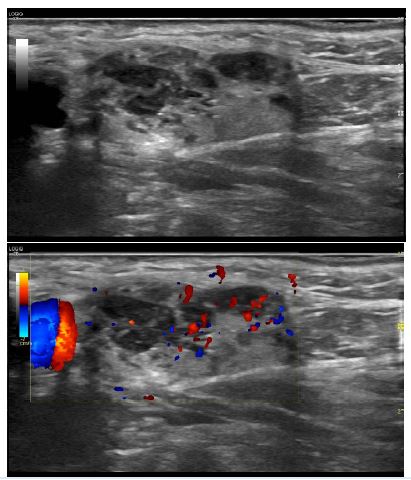
Figure 1: A solid hypoechoic nodule is depicted in the anterior aspect of the salivary gland. The nodule demonstrates central vascularity. On long-axis images multiple nodules can be seen, in addition to the palpable one. The right submandibular gland demonstrates abnormally decreased echogenicity.
Discussion
Küttner’s tumor, otherwise known as chronic sclerosing sialadenitis, is a chronic inflammatory disease of the salivary gland characterized by progressive periductal fibrosis, and acinar atrophy [1,2].
It was first described in 1896 by H. Küttner, who described a series of patients with a unilateral, hard, tumour-like mass of submandibular gland, which histologically showed features of chronic sclerosing sialadenitis [3].
With Kuttners tumor the commonly presenting diagnostic dilemma is that although the lesion is benign, it resembles the clinical features of malignant tumors. When considering that about 80% of all tumors of the submandibular gland are malignant, the management and diagnosis of kuttners tumor is more complicated. Despite the fact that it has been known for more than a century, it is still a rare lesion, but one which must be taken into account in the differential diagnosis of submandibular tumors.
There are numerous theories on the conditions causative agent, one of them is sialolithiasis which is attributed the inflammation and the fibrosis. Other causative agents include the local immune response, secretory dysfunction, ductal anomalies and autoimmune response with the later theory to be prevailing [1,5,6]. Kitawaga et al [2] suggested and studied the involvement of IgG4 antibodies, and its disturbance in the formation of sclerosing sialadenitis [2].
Other authors like Tiemann et al [7] support that Kuttner’s tumor shows the features of an autoimmune process, where the quantity of CD 4 and CD8 positive cells was higher than that of CD3 cells.
Other salivary glands may be involved but upon rare occasions [8-10]. The rarity of the condition means that there are no significant population data to draw safe conclusions on the prevalence in population samples since the literature presents only case series and reports.
The ultrasonographic exam of the condition is not thoroughly analyzed in the literature and in few cases where ultrasonography was performed, the lesions are mentioned as resembling “cirrhotic liver” with diffuse involvement and multiple hypoechoic lesions, together with ductal dilatation and calculi. Doppler shows prominent intraglandular vessels, with no evidence of displacement. Focal lesions are seen as hypoechoic, heterogeneous masses with a radial branching vascular pattern within [10].
Upon a more detailed examination with the current features of ultrasonography performed, the authors report, a hypoechoic nodule on the front surface of the submandibular gland, with a solid texture and the presence of central vasculature. This is a typical case of a “Kuttner tumor” The differential diagnosis includes other autoimmune or not sialadenitis, Mikulicz’s syndrome, benign lymphoepithelial lesion, extranodal marginal zone B-cell lymphoma of MALT [10], inflammatory pseudotumour, fibrohistiocytic tumors, sclerosing lymphoma, sarcoidosis and neoplasms of the salivary glands [2,4,10]. Several associations have been reported, such as sclerosing cholangitis or sclerosing pancreatitis as in the first case studied [2]. In the latter the presence of IgG4 is again another indicator of the relation between the two entities [2].
Upon other radiographic examinations and more particularly MRI in the literature are mentioned as T1: slightly hypointense and T2, STIR and DWI: slightly hyperintense [2].
The management of the lesions can in a few cases be conservative with a follow up recommendation mostly in cases where the mass is not symptomatic (though in many case the benign origin of the lesion should be verified with FNA.Chou et al [6] suggested colour Doppler sonography and sonographically guided needle biopsy as an adequate means of diagnosis, which avoids operative excision of an otherwise benign condition.
Conclusion
Küttner’s tumor is a rare disease, which mimics malignancy. There is not enough evidence to support any diagnostic means that could help in the differential diagnosis of this benign condition. Given the high rate of malignancy in firm, painless lesions of the submandibular gland, surgical excision is often advocated and Küttner’s tumor is usually diagnosed by the histopathologist.
References
- Roh JL, Kim JM. Küttner’s tumor: Unusual presentation with bilateral involvement of the lacrimal and submandibular glands. Act Oto Laryngol. 2005; 125: 792-796.
- Kitawaga S, Zen Y, Harada K. Abundant IgG4-positive plasma cell infiltration characterizes chronic sclerosing sialadenitis (Küttner’s tumor). Am J Surg Pathol. 2005; 29:783-791.
- Küttner H. Überentzundiche Tumoren der Submanxillar-speicheldruse. Bruns BietrKlinChir. 1896; 15: 815-834.
- Huang C, Damrose E, Bhuta S, Abemayor E. Küttnertumour (chronic sclerosing sialadenitis). Am J Otolaryngol. 2002; 23: 394-7.
- Teymoortash A, Tiemann M, Schrader C, Werner J. Chronic sclerosing sialadenitis of the submandibular gland is not just a severe chronic sialadenitis. Am J Otolaryngol. 2003; 24: 278.
- Chou YH, Tiu CM, Li WY. Chronic sclerosing sialadenitis of the parotid gland. J Ultrasound Med. 2005; 24: 551-555.
- Tiemann M, Teymoortash A, Schrader C. Chronic sclerosing sialadenitis of the submandibular gland is mainly due to a T lymphocyte immune reaction. Mod Pathol. 2002; 15: 845-852.
- Blanco M, Mesko T, Cura M. Chronic sclerosing sialadenitis (Küttner’s tumor): unusual presentation with bilateral involvement of major and minor salivary glands. Ann Diag Pathol. 2003; 7: 25-30.
- DeVicente JC, Lopez-Arranz E, Carcia J. Chronic sclerosing sialadenitis of the parotid gland. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 96: 77-80.